A 22 Year Male with Pancreatic pseudocyst
General medicine E - LOG Book
Final practical examination : short case
Hall ticket no : 1701006122
This is an online E-log book to discuss our patient de-identified healthdata shared after taking his/ her guardians sign informed consent
Here we discuss our individual patient problems through series of inputs from available Global online community of experts with an aimto solve those patient clinical problem with collective current bestevidence based inputs.
This E-log also reflects my patient centered online learning portfolio. I have been given this case to solve in an attempt to understand thetopic of " Patient clinical data analysis" to develop my competancy inreading and comprehending clinical data including history, clinicalfinding, investigations and come up with a diagnosis and treatmentplan.
Case presentation :
A 22 year old male,painter by occupation presented with complaint of abdominal pain since 4 days.
History of present illness:
Patient was apparently asymptomatic 4 months back then he developed epigastric pain and vomiting on presenting to a hospital diagnosed as Acute Pancreatitis. He was treated at the hospital and was discharged with the advice to stop drinking alcohol.
4 days back , he developed pain over upper abdomen which is of dragging type, radiating to back aggravated after meals and on lying down(prone>supine)position
Patient denies history of fever, nausea, and diarrhoea.
Patient initially desired to show up for alcohol de-addiction,but was eventually referred to medical opd being syptomatic for pain.
Past History:
Not a known case of Diabetes mellitus, Hypertension. Epilepsy, Cardiovascular diseases. Asthma and tuberculosis
Family History:
No similar complaints in family.
Not significant
Personal history:
Takes mixed diet,
Appetite:Reduced (Early satiety)
Sleep is Adequate.
Bowel and bladder habits are regular
Addictions: Started drinking alcohol 3 years back with friends and later the amount of alcohol incresed to 12 units.
1 Unit=10ml
alcohol daily since 3 years.
Reduced intake to 5 units since 3 months. Last intake was 5 days back of about 8 units of alcohol.
Smokes 7-8 beedies per day
General physical examination: Patient is conscious, coherent,cooperative and well oriented to time, place and person.He is of thin built.
There is no pallor.
No signs of icterus, cyanosis, clubbing lymphadenopathy
edema - present
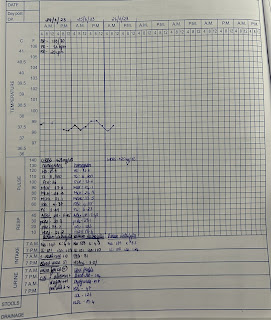
Vitals:
Patient is afebrile
Pulse rate: 92 bpm
Blood pressure: 110/80 mm of Hg
Respirtaory rate: 14 cpm
Systemic Examination:
ABDOMEN EXAMINATION:
INSPECTION:
Shape – Flat
Umbilicus –central in position
All quadrants of abdomen are moving equally with respiration.
No dilated veins, hernial orifices, sinuses
No visible pulsations.
Patient had a swelling left costal border slightly medial to midline .

Not moving with respiration.


PALPATION:
Slight local rise of temperature on left side and no tenderness
All inspectory findings are confirmed.
No guarding, rigidity
Deep palpation- no organomegaly.
PERCUSSION:
There is no fluid thrill , shifting dullness.
Percussion over abdomen- tympanic note heard.
AUSCULTATION:
Bowel sounds are heard.
Provisional diagnosis:Acute fluid collection in pancreas
Investigations:
Serum Lipase: 112 IU/L (13-60)
Serum Amylase: 255IU/L (25-140)
Hemogram:
Hemoglobin: 11.8 mg/dl
Total leucocytes: 14,300 cells/cumm
Lymphocytes: 16(18-20)









diagnosis(confirmed from USG): Pseudocyst of pancreas
Treatment:
Nill Per Oral
Intravenous fluids Ringer lactate and normal saline 10ml per hour
Inj. TRAMADOL 100 mg in 100ml normal saline IV BD
INJ. ZOFER 4mg IV BD
INJ. PAN 40 MG IV BD
INJ. OPTINEURIN 1amp in 100 ml nd IV OD
Psychiatric medication:
TAB. LORAZEPAM 2mg BD
TAB. BENZOTHIAMINE 100mg OD