45/M Left sided limb weakness , Right sided Mouth Deviation
June 01, 2023
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CONSENT AND DE-IDENTIFICATION :
The patient and the attenders have been adequately informed about this documentation and privacy of the patient is being entirely conserved. No identifiers shall be revealed through out the piece of work whatsoever.
Sequence of events:
2013- patient had complaints of polyuria ,went to hospital and was diagnosed diabetic.
Joint pains since 1week which was relieved on medication.
H/o of occasional shock like pain along shoulder(lt)since 6 months.
Patient was brought to causualty with c/o deviation of mouth to right side since yesterday night ,weakness of left upper limb and lower limb since morning ,patient was apparently asymptomatic till yesterday night ,then deviation of mouth towards right side and today morning patient had difficulty walking due to which they visited a local hospital and was treated conservatively and symptoms did not subside and weakness progressed
No h/o slurring of speech ,drooling of saliva
No h/o loss of consciousness,nystagmus,
No h/o head trauma
H/o fever ,low grade since 2days not associated with cough ,headache ,vomitings
H/o alcohol consumption since 15years
K/c/o DM since 10years on tab glimi twice daily
N/k/c/o HTN(180/110)@admission ,CAD ,thyroid epilepsy.


Personal history:
Diet: mixed
Appetite: normal
Sleep: Adequate
Bowel and bladder: Regular
Alcohol intake since 15-20 years (180 ml per day)
GENERAL EXAMINATION:
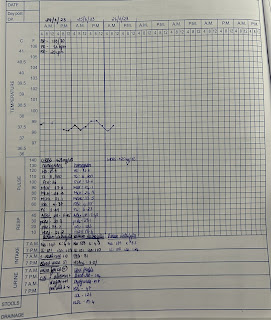
Vitals:
PR-105 bpm
RR- 25 cpm
Temp-99F
Bp-180/110 mmhg
Spo2-98 RA
GRBS-204 mg/dl
No pallor,No icterus, cyanosis, clubbing, lymphadenopathy,edema.
SYSTEMIC EXAMINATION ::
GIT
INSPECTION :
Abdomen - scaphoid
Umbilicus - inverted
Movements - all quadrants are equally moving with respiration.
No scars and sinuses
No visible peristalsis
No engorged veins.
PALPATION:
No local rise in temperature and no tenderness in all quadrants
LIVER: no hepatomegly
SPLEEN- not enlarged
KIDNEYS - bimanual palpable kidneys
PERCUSSION :
no shifting dullness
AUSCULTATION :
Bowel sounds are heard and are normal
No bruit
Respiratory system:
Inspection:
No tracheal deviation
Chest bilaterally symmetrical with pectum excavatum
Type of respiration: thoraco abdominal.
No dilated veins,pulsations,scars, sinuses.
No drooping of shoulder.
Palpation:
No tracheal deviation
Apex beat- 5th intercoastal space,medial to midclavicular line.
Tenderness over chestwall- absent.
Vocal fremitus- normal on both sides.
Percussion:
Supraclavicular
Infraclavicular.
Mammary
Axillary
Infraaxillary
Suprascapular
Infrascapular
Interscapular
Right side and left side- resonant in above areas.
Auscultation:
Bilateral Airway entry - present
Cardiovascular system:
Inspection : no visible pulsation , no visible apex beat , no visible scars.
Palpation: all pulses felt , apex beat felt.
Percussion: heart borders normal.
Auscultation:
Mitral area, tricuspid area, pulmonary area, aortic area- S1,S2 heard.
Central Nervous system:
Higher motor functions- Intact
Cranial nerve functions - Rt.Lower facial nerve weakness +[mouth deviation to Rt.]
Sensory system-Normal(fine and crude touch, proprioception,vibration)
Motor system. Right Left
Power- UL 4/5 1/5
LL 4/5 1/5
Neck N N
Trunk muscles Normal
Tone- UL Normal decrease
LL Normal Decrease
Reflexes-
Superficial reflexes - Intact
Plantar flexion extension
Deep tendon reflexes -
Biceps ++ +++
Triceps ++ +++
Supinator + ++
Knee ++ + ++
Ankle + ++
Cerebellum
Romberg: negative
Finger nose in coordination :absent
Dysdidokinesia : absent
INVESTIGATIONS:













DIAGNOSIS:LEFT HEMIPARESIS 2o TO ACUTE INFARCT IN RT. MCA TERRITORY -MAINLY FRONTO PARIETAL OPERCULUM,PARIETO OCCIPITAL REGION ,INSULAR CORTEX , ADJACENT CORONA RADIATA;K/c/o Dm2 SINCE 10 YEARS.
TREATMENT :1. RT FEEDS 100 ml 2nd hourly
MILK + PROTEIN POWDER 4 th hourly
2.IV FLUIDS NS @ 25ml/hr
3.INJ. THIAMINE 200 mg in 100 ml NS IV BD
4.INJ HAI ACC TO GRBS
5.TAB.ECOSPIRIN-AV (75/10)PO HS
6. TAB. AMLODIPINE 5mg PO/OD 8 am
7.TAB. DOLO 650MG PO SOS
8.T.LORAZEPAM 2mg
9.T. BACLOFEN XL 20 mg